Lower limb development and normal variants - When to Refer
There are a number of common foot and lower limb deformities seen in children. Occasionally presenting symptoms are warning signs that there may be underlying pathology present.
Advice is given below on when and when not to refer for some of the common normal variants.
Referral pathways will depend on local services available but often concerns regarding normal variants will be referred to paediatric orthopaedics, paediatric physiotherapy, community paediatrics or paediatric rheumatology.
A validated Model of Care involving triage (called RightPath) includes a triage guide for normal variants; further information is available.
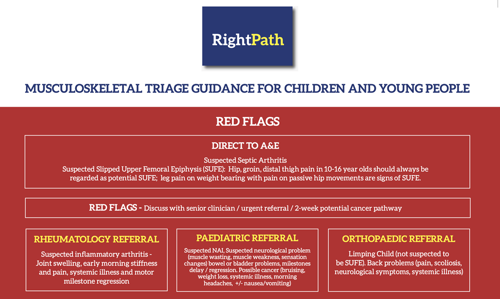
https://www.rightpath.solutions
TOE WALKING - Consider referral if:
- Toe-walking is persistent beyond 2 years.
- There is associated developmental delay.
- The child is unable to squat or stand with their heels on the floor (tightness of calf muscles).
- The child is over 3 years and is unable to stand from floor sitting without using their hands.
- The toe walking is asymmetrical.
Toe walking: Referral is not necessary if: The toe walking is intermittent or can be done intentionally by the child 'for fun' or the child is able to squat to play on the floor and is able to keep their heels on the floor.
FLAT FEET - Consider referral if:
- There are signs of abnormal pressure on the skin of the foot e.g., blistering or callosities.
- The longitudinal arch does not form normally when the child stands on tip-toe.
- The foot is stiff (i.e., the normal arch does not form when the child stands on tip-toe, or the big toe is passively extended).
Flat Feet: Referral is not necessary if: The child is under four years of age, the longitudinal arch forms normally when the child stands on tip-toe or when the big toe is passively extended (i.e., flexible flat feet).
PES CAVUS - This is usually indicative of a neurological cause; therefore a referral to paediatric neurologist or paediatrician is the most appropriate action.
KNOCK KNEES (Genu Valgum) - This is when a child stands with their knees together and their ankles at least 2.5cm apart (intermalleolar distance). A gap of 6 – 7 cm between the ankles (intermalleolar distance) is normal between the ages of two and four years. Knock-knees usually resolve spontaneously approximately by the age of six years.
Consider referral if:
- The problem is associated with pain in the lower limbs.
- The problem is asymmetrical.
- The gap between the ankles is in excess of 6-7 cm.
Knock knees: Referral is not necessary if: The child is under the age of six and the problem does not result in any pain.
BOW LEGS (Genu Varum) - This is when there is a small gap between a child’s knees and the ankles when standing with the feet together. This is normally seen in children until the age of two years. Physiotherapy referral is generally not appropriate. Children are born bow-legged and it approaches normal by 2 years, typically as a result of the child beginning to walk.
Consider referral if:
- There is associated pain in the lower limbs.
- The problem is persistent or asymmetrical.
- The child has evidence of underlying metabolic disease (e.g., Rickets).
IN-TOEING is when a child walks with their feet turning inwards, and is commonly referred to as ‘pigeon toeing’. It is a variation of normal and is part of normal development for many toddlers when just learning to walk. It will usually resolve as the child grows and the musculoskeletal system matures, normally by the age of ten years. During this period of in-toeing the child may tend to trip and fall a little more than their peer group. Insoles and exercises will not help. Surgery is reserved for children over ten years old, or with associated deformities not in keeping with normal variants.
OUT-TOEING is when a child’s feet point outwards. Out-toeing in an adolescent is common; the hips have normal range of movement and are pain free. This condition will usually resolve spontaneously by the age of four and therefore referral is generally not necessary. Urgent referral is needed with recent onset out-toeing in a teenager may be serious and an indication of Slipped Upper (Capital) Femoral Epiphysis). This may associate with limp or pain in the hip or with referred pain in the thigh or knee.
CURLY / CROSSED TOES - Surgery is the only treatment and is usually done in those over 4 years of age. Physiotherapy and podiatry will not help.
DELAYED WALKING - There is considerable variation in the way normal gait patterns develop - such variation may be familial (e.g., ‘bottom-shufflers’ often walk later) and subject to racial variation (e.g., African black children tend to walk sooner and Asian children later than average).
Consider referral if :
- Walking is delayed beyond 18 months.
- Delay in other milestones (e.g., speech, communication, feeding).
- Clumsiness or prone to falling.
- Family history of delayed walking or muscle disease.
- Muscles appear 'bulky' (e.g., calf pseudohypertrophy).
- Difficulty getting up from the floor (Gower's sign).
CLUBFOOT (Congenital talipes equinovarus - CTEV) - All babies born with a talipes equinovarus should be examined by a paediatrician or paediatric physiotherapist, to distinguish whether the deformity is structural or positional in nature. Those with a structural clubfoot should be referred to a specialist paediatric orthopaedic team, who can commence treatment as soon as possible. If the foot position is found to be flexible, assessment should be sought from a paediatric physiotherapist, who can provide appropriate advice and stretches as necessary.